We speak often on this platform about the two faces of our Digital Society. On one side is the promise: artificial intelligence, connectivity and data-driven services opening up opportunities that were unthinkable a decade ago. On the other side are the harms we track every week — cyber threats, online abuse, misinformation, privacy erosion, digital addiction and the misuse of AI. Protecting people in this environment demands that we pay equal attention to digital safety and to digital wellbeing. Safety without wellbeing leaves people protected but disconnected; wellbeing without safety cannot be sustained.
It is against this backdrop that I am glad to draw the attention of readers to the World Summit on Digital Wellbeing (WSDW-2026), an online International Conference being organised by the Council for Digital Safety and Wellbeing (CDSW). I have been associated with this initiative in an advisory capacity, and I believe it deserves the participation of our community of researchers, professionals and policy thinkers.
About the organisers
The Council for Digital Safety and Wellbeing (CDSW) was established in 2026 to advance digital safety and digital wellbeing through research, education, public awareness and policy engagement. It builds on more than a decade of voluntary work carried out through the End Now Foundation, and it brings together researchers, educators, industry, government and civil society to promote the safe, responsible and human-centred use of digital technologies.
The Summit at a glance
- What: World Summit on Digital Wellbeing (WSDW-2026) — an online International Conference
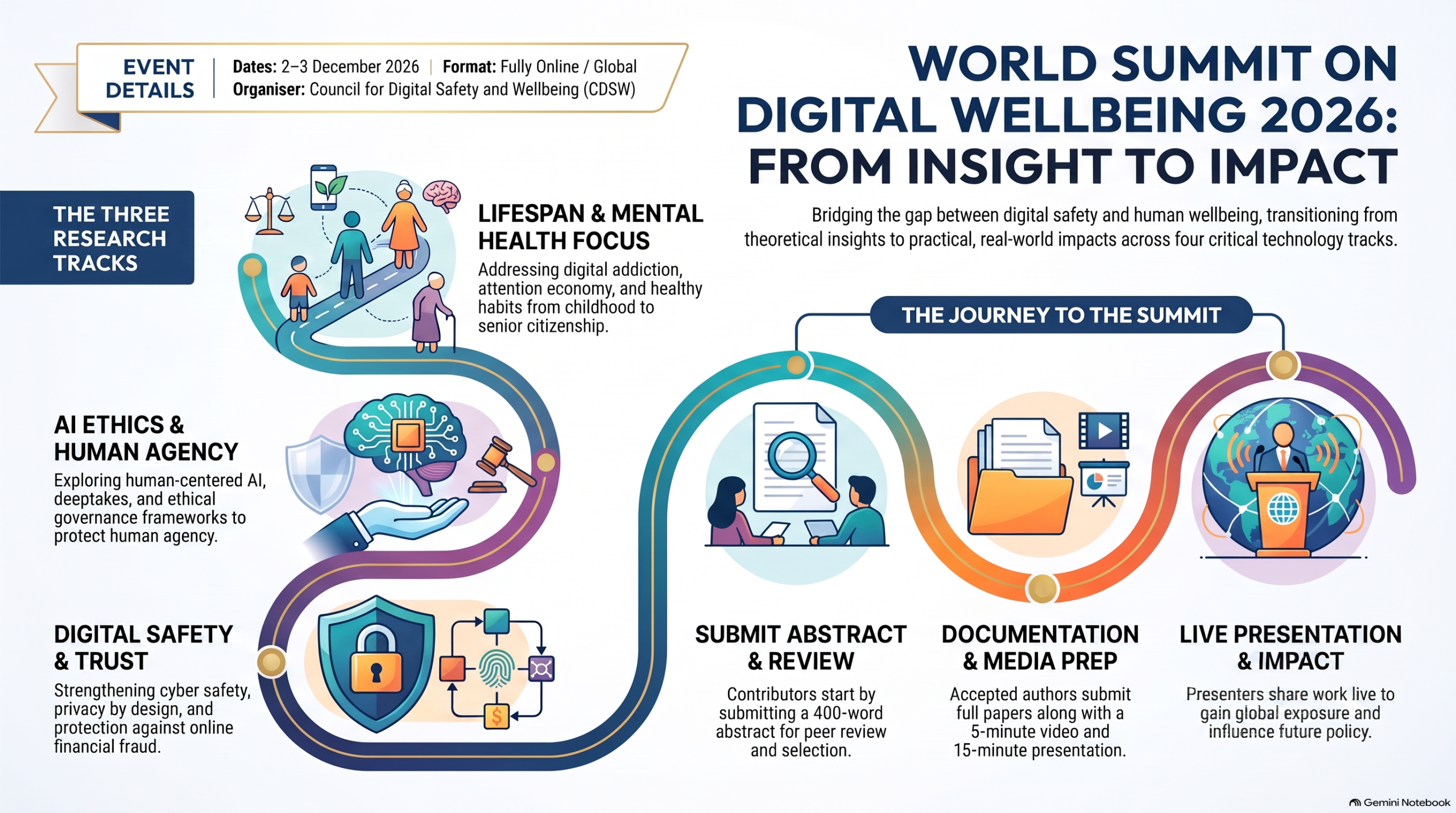
- Theme: Digital Wellbeing: From Insight to Impact
- When: 2–3 December 2026
- Where: Fully online, open to a global audience
The Summit will bring together researchers, practitioners, policymakers, industry leaders, educators and civil society organisations to examine emerging challenges, share evidence-based research, and develop practical solutions for building a safer and healthier digital society.
Four Conference Tracks
Original research papers, case studies, policy analyses and interdisciplinary contributions are invited across four tracks:
-
Digital Wellbeing Across the Human Lifespan — wellbeing from childhood to senior citizenship, age-specific digital risks and interventions, healthy technology habits across generations, and intergenerational approaches.
-
Mental Health, Attention & Human Flourishing — digital addiction, doomscrolling and compulsive behaviours, the attention economy and cognitive overload, technology and sleep, and building resilience in hyperconnected societies.
-
Artificial Intelligence, Ethics & Human Agency — human-centred AI for wellbeing, behaviour manipulation, deepfakes and synthetic media, linguistic and cultural dimensions, and ethical AI governance frameworks.
-
Digital Safety, Cybersecurity & Trust — cyber safety for citizens, digital identity protection, online fraud and financial safety, and privacy by design and digital rights.
Those of us working on the DPDPA, data governance and AI-governance frameworks will find Tracks 3 and 4 particularly close to our current concerns, but the wellbeing lens across all four tracks is a valuable complement to the compliance conversations we usually have.
Who should participate
Researchers and academics, policymakers and government bodies, industry leaders and technology companies, educators, NGOs and civil society, and mental health professionals — anyone with something to contribute to the digital safety and wellbeing conversation.
How to participate
The journey to the Summit runs through five stages:
- Submit Abstract — a 400-word abstract aligned with one of the four tracks
- Receive Acceptance — abstracts are reviewed and selected candidates are notified
- Submit Full Paper — via the conference portal by the stated deadline
- Upload Video & PPT — a 5-minute video and 15-minute presentation
- Present at Summit — present your work live during the assigned track session on 2–3 December 2026
Please visit cdswindia.org/wsdw2026 for the current submission timeline and portal details, and reach out early if you intend to contribute.
What you gain
- Global exposure — showcase your research to an international audience
- Expert feedback — insights from leading experts and practitioners
- Publication opportunities — selected papers may be considered for publication in partner outlets
- Impact and collaboration — build partnerships toward a safer, healthier digital future
- Influence on policy and practice — work that can inform real-world solutions
Partnering with the Summit
Beyond presenting, organisations can engage as Knowledge Partners, Research Partners, Media Partners, Sponsors or Community Outreach Partners. For partnership enquiries, the organising team can be reached at:
- Dr. Prabhakar Rao Jandhyala, Advisor, CDSW — prabhakar.jandhyala@cdswindia.org
- Dr. Anil Rachamalla, Co-Founder & Chief Mission Officer, CDSW — anil.rachamalla@cdswindia.org
General enquiries: wsdw2026@cdswindia.org · LinkedIn: company/cdswindia · X: CDSW_India
A word from me
Much of my work is spent on the legal and compliance architecture of our Digital Society — the DPDPA, the frameworks for data governance, the responsibilities we place on those who process personal data. WSDW-2026 is a reminder that all of this ultimately exists to protect human beings and their wellbeing. I would encourage students, researchers, professionals and organisations in our community to submit a paper, propose a partnership, or simply attend and lend their voice.
Let us join in shaping the future of Digital Wellbeing.
Naavi




")


